Overview
 The Achilles tendon is the largest tendon in the human body. It connects the calf muscle to the heel bone. However, this tendon is also the most common site of rupture or tendonitis, an inflammation of the tendon due to overuse. Achilles tendon rupture is a partial or complete tear of the Achilles tendon. It comes on suddenly, sometimes with a popping sound, and can be debilitating. A full rupture is more severe, but less common, than a partial rupture. A full rupture splits the Achilles tendon so that it no longer connects the calf muscle to the heel: the calf muscle can no longer cause the foot to push off, so normal walking is impossible. If it is a full rupture, then lightly pinching the Achilles tendon with the forefinger and thumb will reveal a gap in the Achilles tendon. Partial and full Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Partial Achilles tendon tears are also common among middle and long distance runners.
The Achilles tendon is the largest tendon in the human body. It connects the calf muscle to the heel bone. However, this tendon is also the most common site of rupture or tendonitis, an inflammation of the tendon due to overuse. Achilles tendon rupture is a partial or complete tear of the Achilles tendon. It comes on suddenly, sometimes with a popping sound, and can be debilitating. A full rupture is more severe, but less common, than a partial rupture. A full rupture splits the Achilles tendon so that it no longer connects the calf muscle to the heel: the calf muscle can no longer cause the foot to push off, so normal walking is impossible. If it is a full rupture, then lightly pinching the Achilles tendon with the forefinger and thumb will reveal a gap in the Achilles tendon. Partial and full Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Partial Achilles tendon tears are also common among middle and long distance runners.
Causes
Inflammation/strain of the tendon is usually caused by overuse, for example, frequent jumping in volleyball, netball or basketball. It is often also caused by a sudden increase in certain types of training, such as hill sprinting or track running, particularly when running in spikes. Tendinopathy can also be associated with ageing. Our ability to regenerate damaged tissue decreases as we age and the quality of the tendon deteriorates. However, the better news is that sensible training can actually strengthen all our soft tissue (tendons, ligaments and muscle). Tightness in the calf muscles will demand greater flexibility of the tendon, which inevitably results in overuse and injury. Biomechanically, the tightness can reduce the range of dorsiflexion (toe up position) in the ankle, which increases the amount and duration of pronation. This problem is known as overpronation.* This reduces the ability of the foot to become a rigid lever at push off and places more lateral and linear forces through the tendon. This imbalance can translate into altered rotation of the tibia (shin bone) at the knee joint and, in turn, produce compensatory rotation at the hip joint with subsequent injuries to the shin, knee and hip. Pronation is part of the natural movement of the subtalar joint in the foot. It allows eversion (turning the sole outwards), dorsiflexion and abduction (pointing the toes out to the side). Pronation is a normal part of the gait cycle, when walking and running, and it helps to provide shock absorption in the foot. When pronation is excessive, the foot has a tendency to roll inward more than normally acceptable. One sign of overpronation is greater wear on the inside of your running shoes than on the midsole. Lack of stability around the ankle joint can also be a contributory factor, as recurrent ankle sprains appear to be associated with a high incidence of Achilles tendonopathy. Wearing shoes that dont fit or support the foot properly can be a major contributing cause of Achilles tendon injury.
Symptoms
Symptoms of an Achilles tendon rupture usually directly follow a traumatic event where the foot is forced in an upward position at the ankle, causing a sudden tight stretch of the Achilles tendon. There can also be a direct blow to the tendon causing a rupture. There is typically a popping feeling or even a popping sound described during the occurance of the rupture. Typically there is pain with swelling in the region. Often the patient is unable to put weight on this foot as there is too much pain.
Diagnosis
When Achilles tendon injury is suspected, the entire lower lag is examined for swelling, bruising, and tenderness. If there is a full rupture, a gap in the tendon may be noted. Patients will not be able to stand on the toes if there is a complete Achilles tendon rupture. Several tests can be performed to look for Achilles tendon rupture. One of the most widely used tests is called the Thompson test. The patient is asked to lie down on the stomach and the examiner squeezes the calf area. In normal people, this leads to flexion of the foot. With Achilles tendon injury, this movement is not seen.
Non Surgical Treatment
Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.
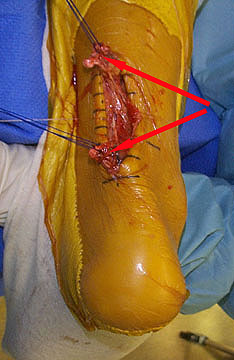
Surgical Treatment
Some surgeons feel an early surgical repair of the tendon is beneficial. The surgical option was long thought to offer a significantly smaller risk of re-rupture compared to traditional non-operative management (5% vs 15%). Of course, surgery imposes higher relative risks of perioperative mortality and morbidity e.g. infection including MRSA, bleeding, deep vein thrombosis, lingering anesthesia effects, etc.
The Achilles tendon is the largest tendon in the human body. It connects the calf muscle to the heel bone. However, this tendon is also the most common site of rupture or tendonitis, an inflammation of the tendon due to overuse. Achilles tendon rupture is a partial or complete tear of the Achilles tendon. It comes on suddenly, sometimes with a popping sound, and can be debilitating. A full rupture is more severe, but less common, than a partial rupture. A full rupture splits the Achilles tendon so that it no longer connects the calf muscle to the heel: the calf muscle can no longer cause the foot to push off, so normal walking is impossible. If it is a full rupture, then lightly pinching the Achilles tendon with the forefinger and thumb will reveal a gap in the Achilles tendon. Partial and full Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Partial Achilles tendon tears are also common among middle and long distance runners.Causes
Inflammation/strain of the tendon is usually caused by overuse, for example, frequent jumping in volleyball, netball or basketball. It is often also caused by a sudden increase in certain types of training, such as hill sprinting or track running, particularly when running in spikes. Tendinopathy can also be associated with ageing. Our ability to regenerate damaged tissue decreases as we age and the quality of the tendon deteriorates. However, the better news is that sensible training can actually strengthen all our soft tissue (tendons, ligaments and muscle). Tightness in the calf muscles will demand greater flexibility of the tendon, which inevitably results in overuse and injury. Biomechanically, the tightness can reduce the range of dorsiflexion (toe up position) in the ankle, which increases the amount and duration of pronation. This problem is known as overpronation.* This reduces the ability of the foot to become a rigid lever at push off and places more lateral and linear forces through the tendon. This imbalance can translate into altered rotation of the tibia (shin bone) at the knee joint and, in turn, produce compensatory rotation at the hip joint with subsequent injuries to the shin, knee and hip. Pronation is part of the natural movement of the subtalar joint in the foot. It allows eversion (turning the sole outwards), dorsiflexion and abduction (pointing the toes out to the side). Pronation is a normal part of the gait cycle, when walking and running, and it helps to provide shock absorption in the foot. When pronation is excessive, the foot has a tendency to roll inward more than normally acceptable. One sign of overpronation is greater wear on the inside of your running shoes than on the midsole. Lack of stability around the ankle joint can also be a contributory factor, as recurrent ankle sprains appear to be associated with a high incidence of Achilles tendonopathy. Wearing shoes that dont fit or support the foot properly can be a major contributing cause of Achilles tendon injury.
Symptoms
Symptoms of an Achilles tendon rupture usually directly follow a traumatic event where the foot is forced in an upward position at the ankle, causing a sudden tight stretch of the Achilles tendon. There can also be a direct blow to the tendon causing a rupture. There is typically a popping feeling or even a popping sound described during the occurance of the rupture. Typically there is pain with swelling in the region. Often the patient is unable to put weight on this foot as there is too much pain.
Diagnosis
When Achilles tendon injury is suspected, the entire lower lag is examined for swelling, bruising, and tenderness. If there is a full rupture, a gap in the tendon may be noted. Patients will not be able to stand on the toes if there is a complete Achilles tendon rupture. Several tests can be performed to look for Achilles tendon rupture. One of the most widely used tests is called the Thompson test. The patient is asked to lie down on the stomach and the examiner squeezes the calf area. In normal people, this leads to flexion of the foot. With Achilles tendon injury, this movement is not seen.
Non Surgical Treatment
Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.
Surgical Treatment
Some surgeons feel an early surgical repair of the tendon is beneficial. The surgical option was long thought to offer a significantly smaller risk of re-rupture compared to traditional non-operative management (5% vs 15%). Of course, surgery imposes higher relative risks of perioperative mortality and morbidity e.g. infection including MRSA, bleeding, deep vein thrombosis, lingering anesthesia effects, etc.
 RSS Feed
RSS Feed